

Rates of Minimally Invasive Surgery After Introduction of Robotic-Assisted Surgery for Common General Surgery Operations

Beyond the Laparoscope: How Robotic Disruption is Democratizing Surgical Access
A retrospective study analyzing trends in general surgery operations found that the adoption of Robotic-Assisted Surgery (RAS) served as a major catalyst for the broader implementation of Minimally Invasive Surgery (MIS). Hospitals that introduced RAS experienced a significantly greater increase in their overall MIS rates compared to non-RAS facilities. This suggests that the investment in advanced surgical platforms is not only changing the method of operation but is also actively driving the diffusion of minimally invasive techniques across common procedures. Crucially, the increase in MIS rates was observed across all analyzed patient populations, including different age groups and insurance payors, pointing to RAS as a powerful force for improving access to less-invasive surgical options.
Futility Thresholds for Emergency General Surgery in the Post–Cardiac Intensive Care Unit

The Cardiac Conundrum: Identifying Futility Thresholds for Post-Surgical GI Catastrophe
This retrospective study of post-cardiac surgery patients requiring Emergency General Surgery (EGS) for gastrointestinal complications, primarily ischemic bowel, revealed a strikingly high 30-day mortality rate of 51%. Analysis identified several critical independent predictors of death: a high Sequential Organ Failure Assessment (SOFA) score, obesity, and thrombocytopenia. Furthermore, the study established laboratory-based futility thresholds—such as platelet count <95 × 10³/μL, lactate >3.4 mmol/L, and elevated bilirubin—beyond which 100% 30-day mortality was observed, providing clinicians with objective metrics to improve risk stratification and guide critical discussions on the appropriateness of EGS interventions in this high-risk post-cardiac surgery population.
Thyroid Surgery Under Nerve Auto-Fluorescence and Artificial Intelligence Tissue Identification Software Guidance
AI-Powered “Fluorescent Vision” Revolutionizes Thyroid Surgery, Eliminating Nerve Damage Risk
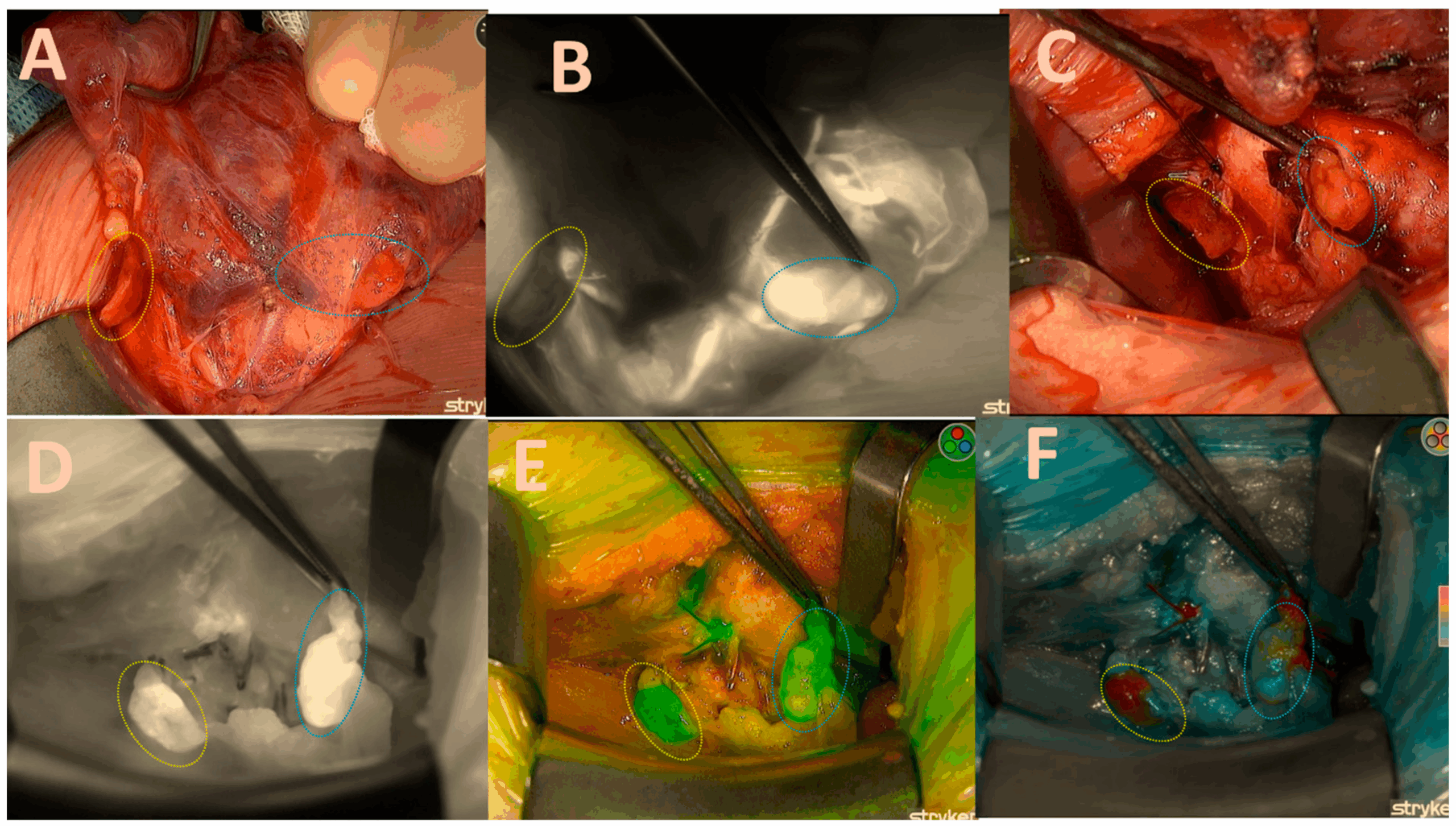
The study presents a significant technological leap in endocrine surgery by addressing the most critical complication of thyroidectomy: recurrent laryngeal nerve (RLN) injury, a feared iatrogenic injury that can result in permanent vocal cord palsies. The research demonstrates the efficacy of a novel surgical system that utilizes nerve autofluorescence technology combined with artificial intelligence tissue identification software to achieve unparalleled intraoperative identification. This handheld device provides surgeons with high-precision visualization and differentiation of the sensory and motor branches of the RLN, which is vital during procedures for conditions like thyroid cancer or a thyroid nodule. By enabling reliable surgical navigation, the findings suggest this innovation can dramatically reduce the risk of intraoperative nerve injuries, thereby improving patient outcomes and establishing a new standard for surgical precision.
Early Use of Norepinephrine in High-risk Patients Undergoing Major Abdominal Surgery: A Randomized Controlled Trial

Proactive Vasopressor Strategy Significantly Lowers Postoperative Morbidity
In this randomized controlled trial evaluating hemodynamic optimization during high-risk major abdominal surgery, researchers demonstrated that a prophylactic continuous intravenous infusion of norepinephrine—a potent vasopressor—significantly outperformed the standard approach of titrated ephedrine boluses in preventing intraoperative hypotension, reducing cumulative episodes from 74% to just 15%. The clinical benefit was profound: the early norepinephrine strategy led to a substantial reduction in the primary endpoint of medico-surgical complications within 30 days (44% versus 58%), suggesting that proactive maintenance of mean arterial pressure during the critical period of anesthesia induction is an effective intervention for minimizing postoperative morbidity and specifically decreasing pulmonary complications in frail surgical populations.
Assessing Surgical Innovation ALPPS: An IDEAL Example of Disruptive Innovation
From Reckless Revolution to Refined Practice: How a Structured Framework Tamed a Radical Surgical Innovation
This analysis demonstrates that the application of the IDEAL (innovation, development, exploration, assessment and long-term) paradigm provided a structured framework for the evaluation and safe integration of the disruptive ALPPS (associating liver partition and portal vein ligation for staged hepatectomy) technique, a high-risk two-stage hepatectomy for previously unresectable liver tumors. In contrast to the initially chaotic adoption of laparoscopic cholecystectomy, which was driven by patient demand and technical fervor despite early safety concerns, and the ongoing industry-promoted diffusion of robotic surgery lacking comprehensive registries, the systematic use of an international ALPPS registry enabled rapid identification of alarming morbidity and mortality. This collaborative data collection facilitated consensus guidelines, refined patient selection, and spurred necessary research, ultimately reducing 90-day mortality from over 15% to below 5% in expert centers and establishing a clear evidence-based pathway for its application.
Robotic vs Laparoscopic Approaches of Pancreatic Resection: A Systematic Review and Meta-Analysis

Robotic or Laparoscopic Pancreatic Surgery: Which Offers Better Outcomes?
This systematic review and meta-analysis, including 46 studies, compared robotic-assisted pancreatic resection (RPR) with laparoscopic pancreatic resection (LPR) in terms of oncological outcomes, perioperative safety, and postoperative recovery. The analysis demonstrated that oncological outcomes and major morbidity were similar between the two approaches, while robotic surgery offered advantages in reducing conversion rates and hospital stay. These findings establish robotic-assisted pancreatic resection as a safe, feasible, and technically favorable minimally invasive approach, though considerations regarding higher costs and resource requirements remain. Future prospective studies and randomized trials are warranted to further define the role and cost-effectiveness of robotic surgery in pancreatic cancer.